Contents
- Healthcare Infrastructure
- The Three-Tiered Structure of the District
- NGOs and Initiatives
- Amhi Amchya Arogyasathi
- Graphs
- Healthcare Facilities and Services
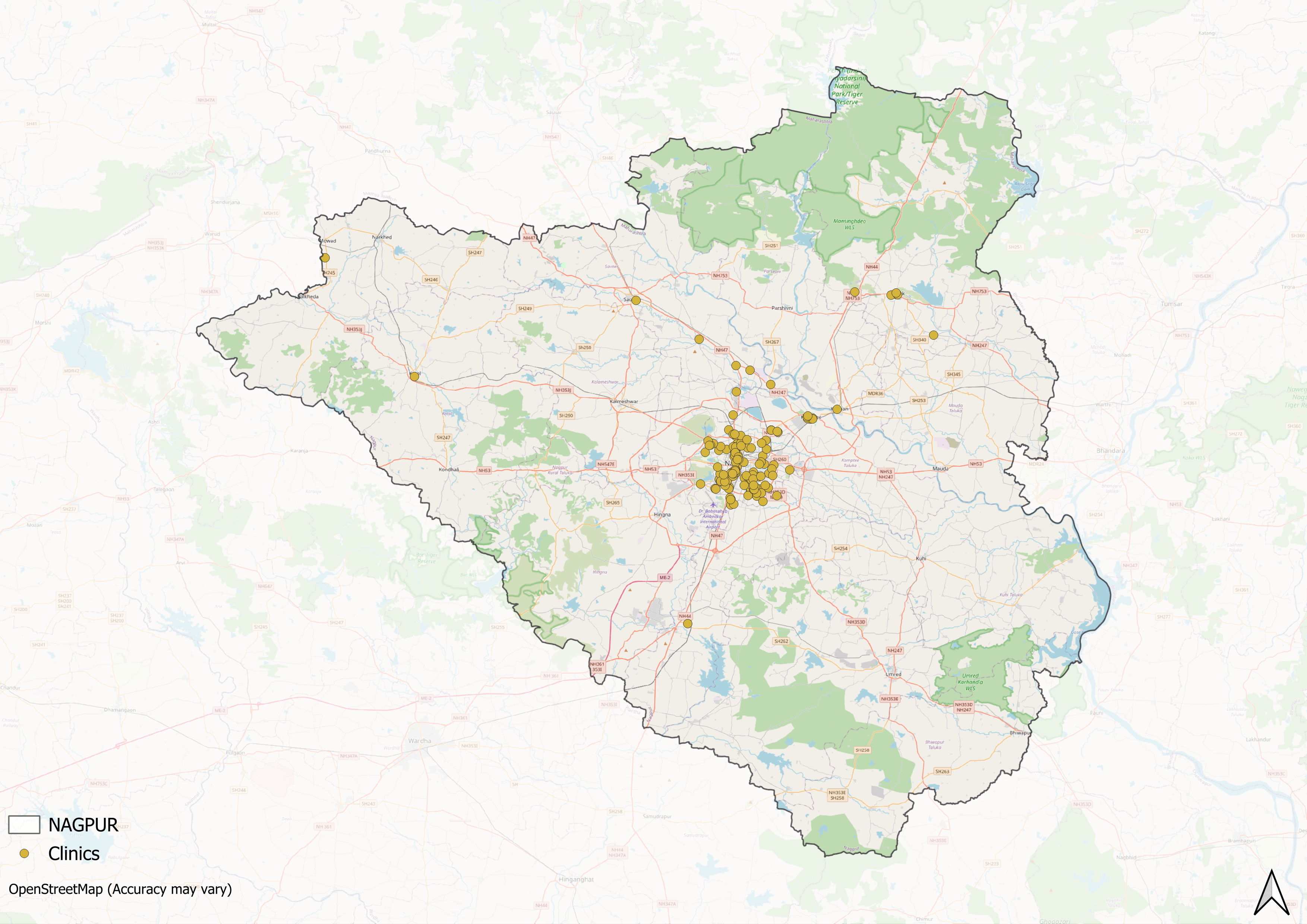
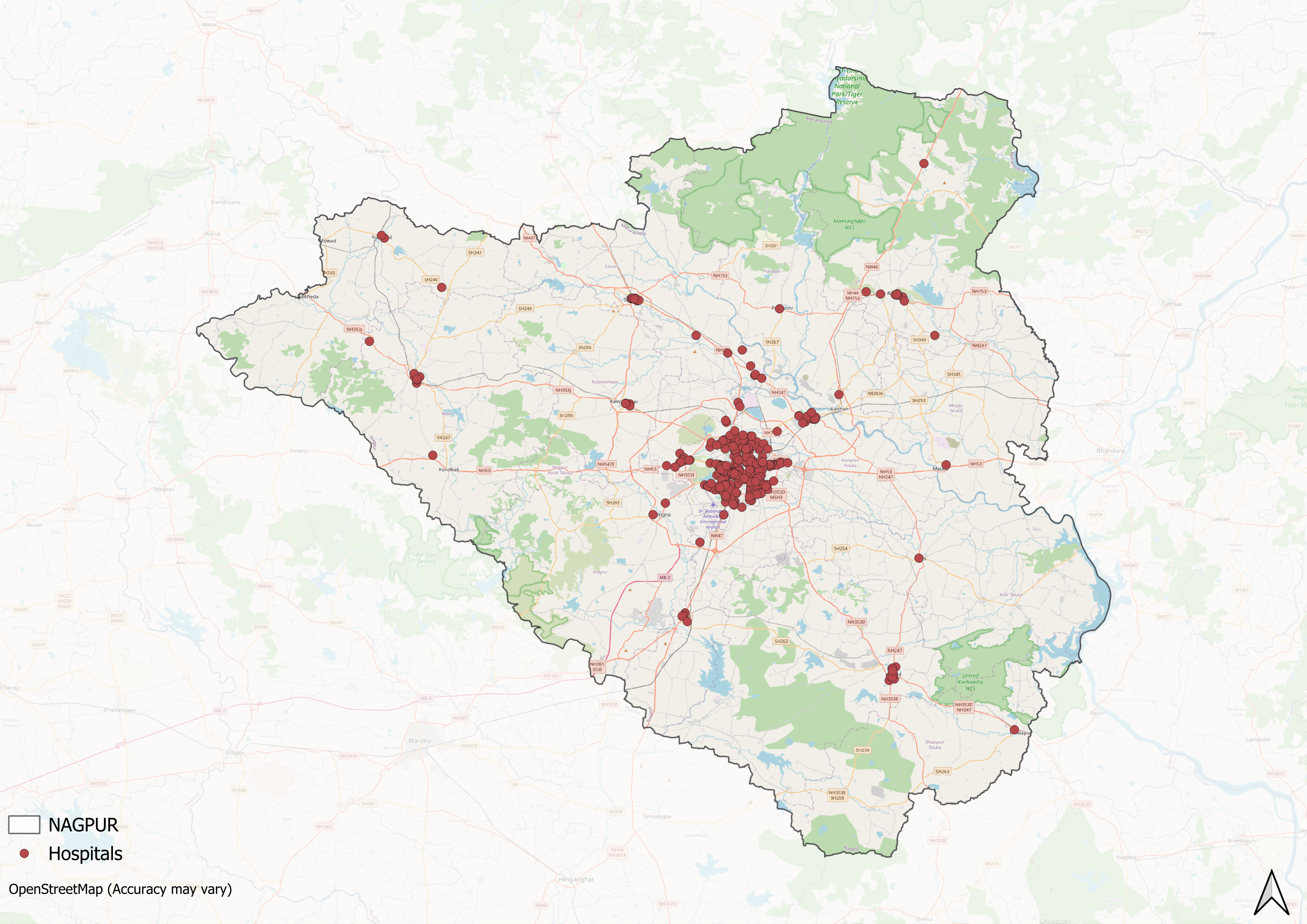
- A. Public and Govt-Aided Medical Facilities
- B. Private Healthcare Facilities
- C. Approved vs Working Anganwadi
- D. Anganwadi Building Types
- E. Anganwadi Workers
- F. Patients in In-Patients Department
- G. Patients in Outpatients Department
- H. Outpatient-to-Inpatient Ratio
- I. Patients Treated in Public Facilities
- J. Operations Conducted
- K. Hysterectomies Performed
- L. Share of Households with Access to Health Amenities
- Morbidity and Mortality
- A. Reported Deaths
- B. Cause of Death
- C. Reported Child and Infant Deaths
- D. Reported Infant Deaths
- E. Select Causes of Infant Death
- F. Number of Children Diseased
- G. Population with High Blood Sugar
- H. Population with Very High Blood Sugar
- I. Population with Mildly Elevated Blood Pressure
- J. Population with Moderately or Severely High Hypertension
- K. Women Examined for Cancer
- L. Alcohol and Tobacco Consumption
- Maternal and Newborn Health
- A. Reported Deliveries
- B. Institutional Births: Public vs Private
- C. Home Births: Skilled vs Non-Skilled Attendants
- D. Live Birth Rate
- E. Still Birth Rate
- F. Maternal Deaths
- G. Registered Births
- H. C-section Deliveries: Public vs Private
- I. Institutional Deliveries through C-Section
- J. Deliveries through C-Section: Public vs Private Facilities
- K. Reported Abortions
- L. Medical Terminations of Pregnancy: Public vs Private
- M. MTPs in Public Institutions before and after 12 Weeks
- N. Average Out of Pocket Expenditure per Delivery in Public Health Facilities
- O. Registrations for Antenatal Care
- P. Antenatal Care Registrations Done in First Trimester
- Q. Iron Folic Acid Consumption Among Pregnant Women
- R. Access to Postnatal Care from Health Personnel Within 2 Days of Delivery
- S. Children Breastfed within One Hour of Birth
- T. Children (6-23 months) Receiving an Adequate Diet
- U. Sex Ratio at Birth
- V. Births Registered with Civil Authority
- W. Institutional Deliveries through C-section
- X. C-section Deliveries: Public vs Private
- Family Planning
- A. Population Using Family Planning Methods
- B. Usage Rate of Select Family Planning Methods
- C. Sterilizations Conducted (Public vs Private Facilities)
- D. Vasectomies
- E. Tubectomies
- F. Contraceptives Distributed
- G. IUD Insertions: Public vs Private
- H. Female Sterilization Rate
- I. Women’s Unmet Need for Family Planning
- J. Fertile Couples in Family Welfare Programs
- K. Family Welfare Centers
- L. Progress of Family Welfare Programs
- Immunization
- A. Vaccinations under the Maternal and Childcare Program
- B. Infants Given the Oral Polio Vaccine
- C. Infants Given the Bacillus Calmette Guerin (BCG) Vaccine
- D. Infants Given Hepatitis Vaccine (Birth Dose)
- E. Infants Given the Pentavalent Vaccines
- F. Infants Given the Measles or Measles Rubella Vaccines
- G. Infants Given the Rotavirus Vaccines
- H. Fully Immunized Children
- I. Adverse Effects of Immunization
- J. Percentage of Children Fully Immunized
- K. Vaccination Rate (Children Aged 12 to 23 months)
- L. Children Primarily Vaccinated in (Public vs Private Health Facilities)
- Nutrition
- A. Children with Nutritional Deficits or Excess
- B. Population Overweight or Obese
- C. Population with Low BMI
- D. Prevalence of Anaemia
- E. Moderately Anaemic Women
- F. Women with Severe Anaemia being Treated at an Institution
- G. Malnourishment Among Infants in Anganwadis
- Sources
NAGPUR
Health
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.
Nagpur’s healthcare landscape, like many other regions across India, is shaped by a mix of indigenous and Western medical practices. For centuries, indigenous knowledge and treatments provided by practitioners such as hakims and vaidyas have formed the foundation of healthcare in the region.
Much of Nagpur’s formal healthcare infrastructure began to take shape under colonial rule with the establishment of the Mayo Hospital in 1867. According to the colonial district Gazetteer (1884), before this, several grant-in-aid dispensaries were also introduced in various zillas, which were among the early efforts to build a healthcare infrastructure within the district. Over the years, the region has witnessed several significant developments in healthcare delivery.
Healthcare Infrastructure
Nagpur’s healthcare infrastructure aligns with the broader Indian model, which is characterized by a multi-tiered system comprising both public and private sectors. Currently, the public healthcare system is tiered into primary, secondary, and tertiary levels. Primary care is provided through Sub Centres and Primary Health Centres (PHCs), while secondary care is managed by Community Health Centres (CHCs) and Sub-District hospitals. Tertiary care, the highest level, includes Medical Colleges and District Hospitals. This system has been shaped and refined over time, influenced by national healthcare reforms.
The Three-Tiered Structure of the District
The district’s formal healthcare network can be traced back to the colonial era. One of the earliest major facilities was Mayo Hospital, established in 1867. Starting as a single-storey structure, it steadily expanded through support from charitable trusts such as the Lady Dufferin Fund. Over the years, Mayo Hospital became an important centre for public health in the region, serving as a base for the Tuberculosis Control and Training Centre and housing an anti-rabies unit. It was also one of the first in the area to introduce blood transfusion services in 1927 and launched a nursing training school when such training was still at an early stage in India.
Medical education in Nagpur gained an early foothold through this same facility. By 1914, a medical school operated at Mayo Hospital under the Nagpur Education Board and offered the L.M.P. Diploma Course, named after Mr. Robertson, then Joint Commissioner of the Central Provinces. Although plans for a full medical college were delayed during World War II, Nagpur University eventually established the Government Medical College in 1948, marking a significant step in strengthening local medical education and specialist care.
![The Government Medical College, established in 1948, strengthened medical education and specialist care in the district, building on the legacy of the earlier medical school at Mayo Hospital.[1]](/media/statistic/images/maharashtra/nagpur/health/the-government-medical-college-established-in_H1Oc9nt.png)
Alongside general and specialist care, Nagpur holds a distinct place in the public mental healthcare landscape of Maharashtra. The Regional Mental Hospital, founded in 1884 as the “Lunatic Asylum.” While the early terminology shows the stigma that shaped mental health treatment at the time, the facility evolved over the decades. The addition of an outpatient wing in 1959 signalled gradual progress in integrating mental health services with general healthcare. Today, the hospital treats over approximately 50,000 patients each year from across Vidarbha — a region grappling with high rates of farmer suicides — and remains one of Maharashtra’s few dedicated mental health institutions providing long-term care.
![Originally founded in 1884 as the Lunatic Asylum, the Regional Mental Hospital is one of Maharashtra’s major facilities providing long-term mental healthcare.[2]](/media/statistic/images/maharashtra/nagpur/health/originally-founded-in-1884-as-the-lunatic-asy_0LA3Tvy.png)
In more recent decades, Nagpur has seen substantial growth in its private healthcare sector. The city has become an important medical hub for patients from neighboring states such as Madhya Pradesh, Jharkhand, and Chhattisgarh. Institutions like Care Hospital, founded in 2006, and the Meditrina Institute of Medical Sciences, established by neurosurgeon Dr. Sameer Paltewar, have added to the city’s advanced care capacity. Meditrina, with its NABH accreditation and ISO certifications, is known for its multispecialty services, including a dialysis unit and modern radiodiagnostics.
![Meditrina Institute of Medical Sciences, Nagpur isa multispecialty hospital founded by Dr. Sameer Paltewar, offering advanced services like dialysis and radiodiagnostics.[3]](/media/statistic/images/maharashtra/nagpur/health/meditrina-institute-of-medical-sciences-nagpu_kVisURF.png)
Chain hospitals like Wockhardt have further expanded Nagpur’s medical offerings, giving residents and visitors access to a wide range of specialized treatments.
NGOs and Initiatives
The determinants of health and health outcomes, as the World Health Organization (WHO) elaborates, are not solely shaped by more than just medical factors and healthcare services. The organization uses the term “social determinants of health (SDH)” to refer to the “non-medical factors that influence health outcomes.” These non-medical factors can be sanitation, nutrition, community well-being, or, as the WHO outlines, “income and social protection,” “food security,” access to quality healthcare, and more.
While there have been ongoing efforts to strengthen Nagpur district’s healthcare infrastructure, certain areas still face challenges, particularly in addressing these broader health determinants. In response, non-governmental organizations have emerged as vital partners, working alongside public health systems to develop innovative, grassroots-level approaches that bridge these gaps.
Amhi Amchya Arogyasathi
Established in 1984 by Dr. Satish Gogulwar and Shubhada Deshmukh, Amhi Amchya Arogyasathi is a Nagpur-based non-governmental organization that works to address health and social challenges faced by local communities, particularly women, tribal groups, and farmers. The organization draws inspiration from Gandhian and Vinoba Bhave’s philosophies, focusing on a holistic approach to well-being that goes beyond medical care to include livelihoods, nutrition, clean water access, and empowerment.
![Community health workers and local women participating in a health awareness rally organized by Amhi Amchya Arogyasathi in Nagpur district.[4]](/media/statistic/images/maharashtra/nagpur/health/community-health-workers-and-local-women-part_ja8ntJl.png)
One of the organization’s core priorities is tackling malnutrition, which remains a significant concern linked to childhood stunting and maternal anemia. Through training local community health workers, known as Arogya Sakhi, the group promotes better nutrition, maternal care, sanitation, and health awareness at the village level.
A notable initiative has been the promotion of Nutri or Kitchen Gardens. This program encourages families to grow vegetables at home, helping to secure a steady supply of nutritious food and to raise awareness about healthy diets. In some cases, the sale of surplus produce has also provided an additional source of income.
Since 2003, the organization has also run a community-based rehabilitation program to support persons with disabilities (PwDs). This effort emerged in response to limited awareness of the rights and resources available to PwDs. By forming Self-Help Groups (SHGs) and federations, the program helps individuals access government schemes, share information, and advocate for their entitlements. Over a thousand PwDs currently participate in these local networks.
Graphs
Healthcare Facilities and Services
Morbidity and Mortality
Maternal and Newborn Health
Family Planning
Immunization
Nutrition
Sources
Arogya Sathi. "What We Do." Arogya Sathi.https://www.arogyasathi.org/what-we-do-page#
Government Medical College, Nagpur. "About GMC Nagpur." GMC Nagpur.https://gmcnagpur.org/about-gmc-nagpur
M Choksi, B. Patil et al. 2016.Health systems in India. Vol 36 (Suppl 3). Journal of Perinatology.https://pmc.ncbi.nlm.nih.gov/articles/PMC514…
Maharashtra State Gazetteers. 1971. Nagpur District Gazetteer, 1st ed. Directorate of Government Printing, Stationery and Publications, Maharashtra State.
Meditrina Institute of Medical Sciences. "Hospital Profile." Meditrina Institute.https://meditrinainstitute.com/hospital-prof…
Samir Nazareth. 2017. "Is Nagpur Living Up to Its Identity as a Medical Hub?" The Quint.https://www.thequint.com/opinion/is-nagpur-l…
Social determinants of health. WHO.https://www.who.int/health-topics/social-det…
Stanza Living. 2023. "Best Hospitals in Nagpur." Stanza Living Blog.https://www.stanzaliving.com/blog/best-hospi…
Varsha Roysam. 2017. "How Tata Trusts Is Giving Nagpur Mental Hospital a Much-Needed Makeover." YourStory.https://yourstory.com/2017/06/nagpur-mental-…
Last updated on 26 July 2025. Help us improve the information on this page by clicking on suggest edits or writing to us.